Qualification pathways in the health occupations and current challenges
Maria Zöller
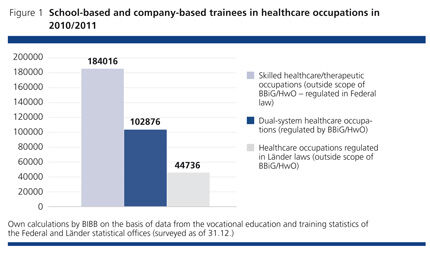
With around 4.8 million employees, the health system is Germany's largest and most expansive growth and employment market. Future challenges are posed by changing care needs resulting from demographic change, and by the growing complexity of care provision and new demands for interprofessional collaboration. These have implications for future qualification requirements and hence also for training and qualification. So what are the existing (training and qualification) pathways into the health service? The article structures and systematises the heterogeneous and confusing landscape of the non-academic training occupations. Starting out from the various legal bases on which these qualifications are regulated, it introduces the relevant initial vocational education and training (IVET) programmes. Currently these account for an approximate total of 330,000 school-based and company-based trainees across the (German vocational education) system (cf. Figure 1). After discussing continuing vocational education and training (CVET) options and current developments, the article concludes with an outlook for the possible further development of vocational education in this sector.
Three vocational training pathways
The health sector is the largest branch in Germany's economy and offers employment and career opportunities in diverse fields of activity. According to the Federal Employment Agency, one in ten employees subject to social security contributions is already working in a healthcare or nursing occupation (cf. BA 2011, p.3). A large number of initial and continuing vocational education and training (IVET & CVET) options are open to young people. These are regulated on various legal bases, from regional laws to the national-level Vocational Training Act (BBiG) and the Crafts and Trades Regulation Code (HwO).
Skilled healthcare/therapeutic occupations (outside scope of BBiG/HwO)
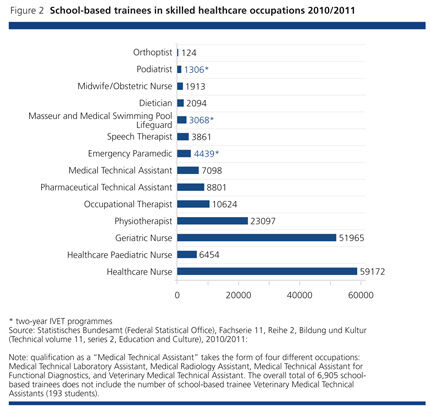
The first and, in numerical terms, largest pillar of training and qualification (183,823 trainees in the academic year 2010/2011) is made up of the 17 skilled healthcare occupations. Training for these healthcare and therapeutic occupations takes place on the basis of the laws regulating the relevant occupations (e.g. "Law on the recognised occupation of the Midwife and Obstetric Nurse (HebG)" or "Law on the recognised occupation of the Occupational Therapist (ErgThG)", and the corresponding training and examination regulations which are regulated in Federal German law. The duration of training in skilled healthcare occupations is three years for most IVET programmes (cf. Figure 2).
Permission, in the form of a license, is necessary to work in one of these therapeutic occupations. Certain conditions attach to the license to use the occupational title, which are laid down in the laws governing the respective occupations (see panel).
Conditions for use of the occupational title
A license to use the occupational title is to be issued on application, if the applicant
- has passed the examination after the specified initial vocational training period,
- has committed no misconduct that casts doubt on his or her reliability to carry on the occupation,
- is not unsuitable to carry on the occupation for health reasons and
- has the necessary German language skills to carry on the activities of the occupation. (cf. § 2 subsection 1 of the relevant occupational laws)
The legislation on admittance to the therapeutic occupations ("Admission to the medical and other therapeutic occupations pursuant to Art. 74 para. 1 no. 19 of the German Basic Law (GG)") falls within the competence of the German Federal Government (cf. Bund-Länder-AG 2012,).
Dual-system occupations in healthcare (regulated by BBiG/HwO)
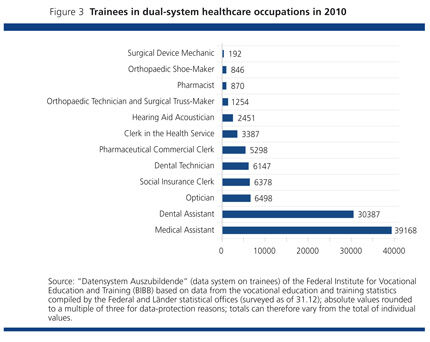
The second pillar of training and qualification (102,876 trainees) is made up of the dual-system healthcare occupations, training for which is regulated on the basis of the Vocational Training Act (BBiG) or the Crafts and Trades Regulation Code (HwO). IVET takes place in the two learning venues of the workplace and the part-time vocational school. It is based on standardised national "training regulations" for workplaces and accompanying "framework curricula" for the school-based element, and normally lasts for 36 months (cf. Figure 3).
Health sector occupations regulated in regional law (outside scope of BBiG/HwO)
The third pillar of training and qualification (44,736 trainees) consists of occupational qualifications regulated in regional law, i.e. on the basis of the Schools Law in each of the German federal states (Länder). The duration of training on these programmes is between 24 and 36 months. Only certain German Länder offer IVET programmes at full-time vocational schools and qualification titles are not necessarily standardised (KMK 2012 a and b). Vocational training for the occupations of Geriatric Care Assistant and Healthcare and Nursing Assistant is offered predominantly in health sector vocational schools. IVET programmes for the occupation of Social Assistant registered the highest number of trainees in the academic year 2010/2011 (cf. Figure 4, p.8).
CVET - a heterogeneous field
CVET in the context of the healthcare system is also very heterogeneous, and requires differentiated consideration relative to the different pillars of IVET. In view of this heterogeneity, the following presentation only refers to regulated programmes of advanced and continuing vocational education with qualifications governed by national or regional laws. Within these parameters, examples of existing CVET options are presented. 01 Regulated CVET in the skilled healthcare (or therapeutic) occupations is characterised by a continuing education structure with either specialised programmes regulated in regional law (including such continuing education qualifications as Specialist Healthcare Nurse for Intensive Care and Anaesthesia, Specialist Healthcare and Paediatric Nurse for Intensive Care and Anaesthesia, or Specialist Healthcare Nurse for Psychiatry), or functional CVET programmes (including the CVET qualification as Head of Nursing or Functional Unit in the Health Service), bearing in mind that qualification titles vary in the individual Länder. For the dual-system occupations of the health sector, CVET is available in the form of "upgrading training" options, which are regulated at Federal Government level. For instance, in the healthcare-specific crafts sector, corresponding Master Craftsperson training programmes are offered (e.g. Master Craftsperson qualification in Vision Optics, Master Craftsperson qualification in Dental Technology, etc.). For Medical and Dental Assistants and those qualified in business-based healthcare occupations, one progression route is an advanced vocational qualification as a Certified Senior Clerk for Healthcare and Social Services, which is regulated at Federal Government level and has been available since 2011. A further option in the health sector is the advanced vocational qualification as a Certified Pharmaceutical Sales Representative, also regulated in Federal law. Other than this, CVET programmes are also offered at trade and technical schools; these vary from one German Land to another and cover specialisations such as Curative Education (cf. KMK 2012 b).
Relevant developments in the health sector
Occupations in the health sector are affected by the demographic trend in two respects: On the one hand, the ageing of the population and the associated shift in the spectrum of ill-health is causing a rising demand for health services, and hence also for skilled staff. On the other hand, the parallel decline in the birth rate means that falling numbers of young people will be embarking on vocational training for a recognised healthcare occupation in future. In geriatric care, the shortage of skilled staff is already apparent and extends to almost all the German Länder. In 2011, advertised positions for qualified geriatric nursing staff remained vacant for 110 days on average across Germany as a whole. Only in the state of Brandenburg were positions filled more quickly (cf. BA 2011, p.16).
In the German Science Council's view, demographic change and the growing proportion of older people, combined with epidemiological changes like the rise in chronic illnesses and multi-morbidity, are leading to a quantitative expansion and quantitative change in care needs. Ageing is generally associated with increasing health problems and the risk of becoming dependent on care. Moreover, chronic illnesses are on the increase even among children and young people. As a result of medical advances and the resulting new opportunities for diagnostics and therapies, the care-provision remit is growing in complexity. Meanwhile the necessity for more cooperative organisation of healthcare poses new challenges for interprofessional collaboration (cf. Wissenschaftsrat 2012, p. 8).
What conclusions can be drawn for vocational training?
In the aim of identifying future changes in qualification demands in the healthcare sector, a study was carried out on behalf of the Federal Ministry of Education and Research (BMBF) on future occupational qualification requirements at the intermediate qualification level in healthcare ("Zukünftige Qualifikationserfordernisse bei beruflichen Tätigkeiten auf mittlerer Qualifikationsebene im Bereich Public Private Health") (cf. INFAS/WIAD 2011). Based on the results of the study published in September 2011, three illustrative aspects are presented which are particularly relevant to vocational training in healthcare occupations involving direct patient contact.
Higher expectations concerning advice and coordination
According to the early-identification study, a wealth of new demands are associated with the expansion of out-patient care structures. Apart from the creation of autonomous coordination services, the importance of advice on neighbourhood care provision is emphasised. Furthermore, it is seen as an indispensable role to advise, guide and support relatives of older people, particularly dementia sufferers (cf. INFAS/WIAD 2011, p. 6). The report also refers to the ability to work in multi-professional teams as becoming increasingly important. It specifies teamwork skills and interprofessional cooperation, but also conflict management and moderation as elements in an important toolkit that needs to be imparted at an early stage, i.e. in the course of IVET. (ibid. 2011, p. 52)
In its current recommendations on higher education qualifications for the health sector, the German Science Council asserts that complexity has risen in the occupational fields of nursing, the therapeutic occupations (physiotherapy, speech therapy, occupational therapy) and midwifery, particularly with regard to patient education and advice, the increasing use of care-supporting technologies, and the management of care (cf. Wissenschaftsrat 2012, p.8).
In the context of further developing the nursing occupations and the planned merging of the three existing IVET programmes in Healthcare and Nursing, Healthcare and Paediatric Nursing and Geriatric Nursing, it also draws attention to the growing importance of the advice and support role as well as the tasks of coordination and evaluation (cf. Bund-Länder-AG 2012, p. 7/29; WEIDNER/ KURTZ, BWP 6/2012).
The rising demands for advice, guidance and coordination place higher expectations upon the social and personal competencies of skilled staff in the health service. Particularly given the context of physically and psychologically demanding care processes, in which the specific needs and concerns of patients of all age-groups must be taken into consideration, skilled staff are often challenged to manage their own resources competently with regard to looking after their own health.
Growing significance of prevention and health promotion
According to the early-identification study, consistent involvement of the skilled healthcare occupations in health promotion and prevention is seen as necessary. In this context it is emphasised that these skilled staff require additional competencies in health psychology which allow them to work collaboratively with their clients to reach a shared communicative reflection and, where appropriate, revision of individual behaviours (INFAS/WIAD 2011, p. 11).
Health promotion, as understood by the World Health Organization (WHO), is a strategy applicable both to the analysis and reinforcement of health resources and human health potential and to all levels of society (multilevel approach). 02 Back in 1986 in the Ottawa Charter on Health Promotion, the World Health Organization formulated the objective of "enabling people to increase control over, and to improve, their health." (WHO 1986, p. 1). In the current health policy discussion, the Federal Ministry for Health (BMG) ascribes vital importance to health promotion for children and young people, and to company-based health promotion.
For the healthcare occupations described, important new tasks and fields of activity could arise in the field of health promotion.
New tasks as work done by doctors is delegated
The Federal Ministry for Health (BMG) refers to neighbourhood medical care as one of the German health system's most important services, but acknowledges that even now, sufficient numbers of doctors are no longer available in all regions (BMG 2011, p. 1). Against this backdrop, the study on future qualification requirements already ventures to suggest that in view of these changes and the growing problem of under-provision in rural regions, new tasks are likely to arise for skilled staff in the non-academic health occupations.
On 22.03.2012 a guideline issued by the Federal Joint Committee (G-BA) specifying which medical tasks could be reassigned to qualified geriatric and healthcare nurses for autonomous provision of medical care within the framework of pilot projects ("Richtlinie über die Festlegung ärztlicher Tätigkeiten zur Übertragung auf Berufsangehörige der Alten-und Krankenpflege zur selbständigen Ausübung von Heilkunde im Rahmen von Modellvorhaben nach § 63 Abs. 3c SGB V") entered into force. It stipulates which tasks medics may delegate to skilled nursing staff in the course of pilot projects.
According to the benchmark paper for the new law on the nursing occupations, in principle it is assumed that nursing staff will acquire the relevant level of qualification to take responsibility for such delegated medical duties during the course of their academic training (cf. Bund-Länder AG 2012, p. 5; WEIDNER/KURTZ, BWP 6/2012).
In the view of the German Science Council, the existing IVET provision for skilled healthcare occupations at vocational schools is no longer adequate to impart the capabilities and expertise that are now required.
"Against the background of an observable increase in complexity in many areas of healthcare, changes in the division of tasks and the increasing importance of interprofessional cooperation, the German Science Council considers it advisable that members of the skilled healthcare occupations, who will be entrusted with particularly complex and responsible tasks, should preferably be university-educated in future (Wissenschaftsrat 2012, p. 81; own translation).
Similarly, the European Commission's proposal to raise the prerequisites for admission to IVET in nursing and midwifery to twelve years of school-based education makes reference to today's higher level of expectations: "The nursing and midwifery professions have significantly evolved in the last three decades: community-based healthcare, the use of more complex therapies and constantly developing technology presuppose a capacity for higher responsibilities for nurses and midwives. [...] Therefore, admission to that training should be increased to twelve years of general education or success in an examination of an equivalent level." (European Commission 2011, p. 19)
Outlook - what can be done?
The health occupations mentioned in the introduction play an essential part in meeting the healthcare needs of the population. Currently changes in the health sector are making new demands upon the occupational qualification levels of employees. The three pillars of training and qualification in non-academic healthcare occupations operate in parallel but largely in isolation from one another, both in the IVET and CVET domains. Varying legal bases and different Länder and Federal Government competencies mean that new developments in the field of vocational education tend to be specific to one particular pillar. Only limited horizontal and vertical permeability exists. One question that remains unanswered is how, amid the competing forces of raised expectations in the employment system, the debated move towards academic training in the skilled healthcare occupations, and developments in the European context, a form of vocational education and training can be designed which meets future needs. Opportunities for modernisation and evolution might best be found by adopting a common orientation towards current and future requirements. Occupational profiles must be reconceived! With a view to optimising healthcare, it is indispensable to have a system of initial and continuing vocational education and training that spans all the divides and is coordinated in terms of occupation-specific tasks and responsibilities - and incorporates new task areas to meet the demands of tomorrow.
Literature
BIBB: "Datensystem Auszubildende" des BIBB auf Basis der Daten der Berufsbildungsstatistik der statistischen Ämter des Bundes und der Länder (surveyed as of 31.12.)
BUNDESAGENTUR FÜR ARBEIT: Arbeitsmarktberichterstattung: Gesundheits-und Pflegeberufe in Deutschland. Nürnberg 2011 - URL: www.statistik.arbeitsagentur.de/Statischer-Content/Arbeitsmarktberichte/Berichte-Broschueren/Arbeitsmarkt/Generische-Publikationen/ Gesundheits-und-Pflegeberufe-Deutschland-2011.pdf (retrieved: 09.10.2012)
BUND-LÄNDER-ARBEITSGRUPPE: "Weiterentwicklung der Pflegeberufe": Eckpunkte zur Vorbereitung des Entwurfs eines neuen Pflegeberufegesetzes vom 01.03.2012. Berlin 2012 - URL: www.bmg.bund.de/fileadmin/dateien/Downloads/P/Pflegeberuf/20120301_Endfassung_Eckpunktepapier_Weiterentwicklung_der_Pflegeberufe.pdf (retrieved: 09.10.2012)
BMG: Für eine gute Versorgung. In: Gesundheitspolitische Informationen (GP) No. 3/2011. Berlin 2011
EU COMMISSION: Proposal for a DIRECTIVE OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL amending Directive 2005/36/EC on the recognition of professional qualifications and
Regulation on administrative cooperation through the Internal Market Information
System. Brussels 19.12.2011, COM (2011) 883 final
INSTITUT FÜR ANGEWANDTE SOZIALWISSENSCHAFT GMBH (INFAS); WISSENSCHAFTLICHES INSTITUT DER ÄRZTE DEUTSCHLANDS (WIAD): Zukünftige Qualifikationserfordernisse bei beruflichen Tätigkeiten auf mittlerer Qualifikationsebene im Bereich Public Private Health. Bonn 2011
KMK: Dokumentation der Kultusministerkonferenz über landesrechtlich geregelte Berufsabschlüsse an Berufsfachschulen (Beschluss des Unterausschusses für Berufliche Bildung vom 26.01.2012) [cit. 2012 a]
KMK: Rahmenvereinbarung über Fachschulen (Beschluss der Kultusministerkonferenz vom 07.11.2002 i. d .F. vom 02.03.2012), Beschluss Nr. 430 - URL: www.kmk.org/fileadmin/veroeffentlichungenbeschluesse/2002/2002_11_07-RV-Fachschulen.pdf (retrieved: 09.10.2012) [cit. 2012 b]
STATISTISCHES BUNDESAMT: Fachserie 11, Reihe 2 Bildung und Kultur. Berufliche Schulen 2010/2011
WHO: Ottawa-Charta zur Gesundheitsförderung 1986 - URL: www.euro.who.int/__data/assets/pdf_file/0006/129534/OttawaCharter_G.pdf (retrieved: 09.10.2012)
WISSENSCHAFTSRAT: Empfehlungen zu hochschulischen Qualifikationen für das Gesundheitswesen. Berlin 2012 - URL: www.wissenschaftsrat.de/download/archiv/2411-12.pdf (retrieved: 09.10.2012)
MARIA ZÖLLER
Research associate in the “Customer Service Occupations, Cross-Cutting Tasks” Division at BIBB
Translation from the German original (published in BWP 6/2012): Deborah Shannon, Academic Text & Translation, Berlin
-
1
For the sake of completeness, mention is made here of the diversity of CVET options not regulated in either national or regional law.
-
2
The five main action areas in health promotion are:
- Developing a health-promoting overall policy,
- Creating health-promoting life-worlds,
- Supporting health-related community campaigns,
- Developing personal competencies and
- Reorientating health services.